Neuro-Ophthalmology & Neuro-Otology
Dizziness
May. 14, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
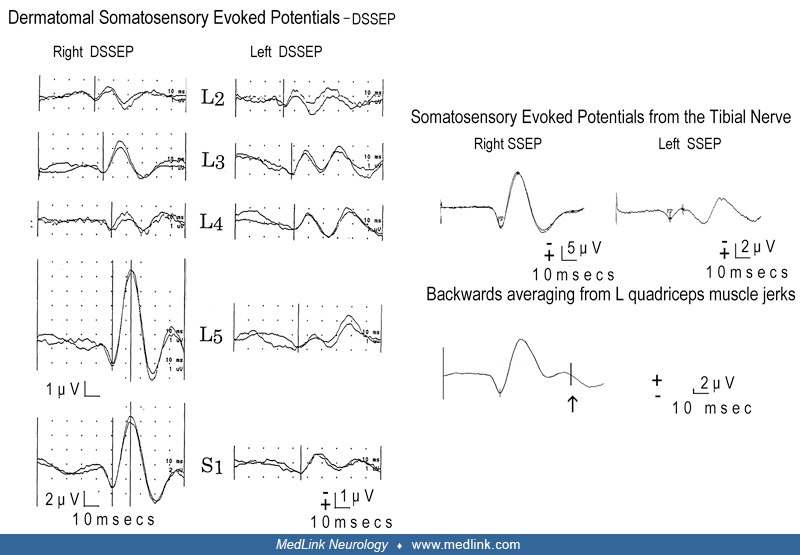
Neurophysiological investigations in a man aged 26 years with onset of epilepsia partialis continua at the age of 25. This consisted of continuous and arrhythmic twitching of various muscles of the left leg and particularly the toes. There was great variation in intensity, spread, and severity. It was exaggerated on dorsiflexion of the foot and improved when resting. On 5 occasions, this progressed in a jacksonian manner to generalized tonic-clonic seizures. The clonic movements of the toes spread to the foot and then to the knee for 5 minutes prior to somatosensory-evoked potentials. On neurologic examination, there were mild pyramidal signs of the left leg. All possible tests to discover the cause of this were negative, including high-resolution MRI and PET scanning and cerebrospinal fluid with appropriate metabolic screening. Mitochondrial disease was also excluded. After a short course of steroids and drug treatment with mainly clonazepam, the situation improved dramatically. Ten years later, he is well, although he has some infrequent clusters of irregular twitching of the toes of the left leg and is still on clonazepam. (A, C) Dermatomal and somatosensory potentials are gigantic on the right side (from stimulation of the left). Note that the maximum amplitude of the dermatomal potentials is obtained when the S1 dermatome is stimulated. (B) C reflex of around 65 ms latency is obtained only from muscles of the left leg stimulating the peroneal nerve (similar responses were also obtained from other left-sided leg muscles by stimulating other left leg nerves or by tapping for the knee jerk). (D) Jerk-locked, back-averaged cortical potentials appear in the contralateral primary motor area preceding the jerks by 25 ms (positive peak). (Contributed by Dr. C P Panayiotopoulos.)