Headache & Pain
Headache in transplant patients
Jul. 29, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
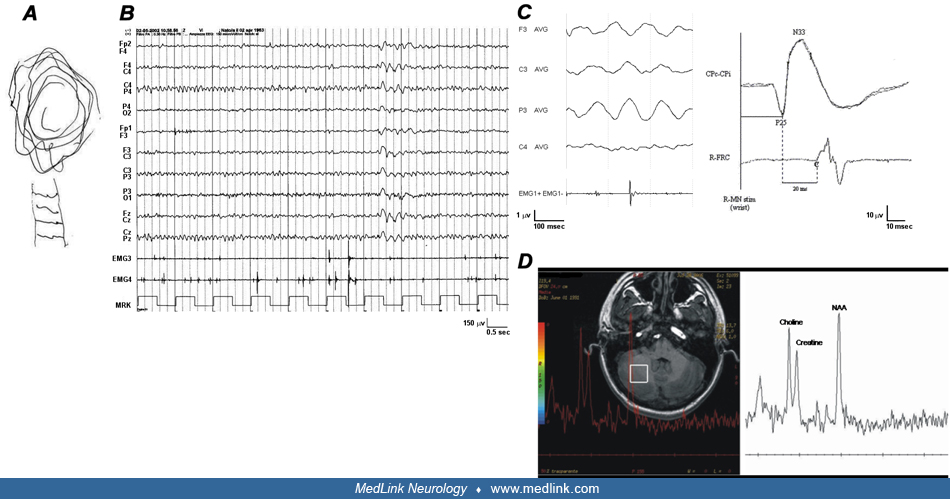
Electroclinical and MRI features in a patient with BAFME. (A) Free-hand drawing showing cortical tremor; the drawing is perturbed by sudden, brisk jerks, highly suggestive of myoclonus. (B) Polygraphic recording showing mild, generalized paroxysmal activity and irregular, short-lasting electromyographic bursts, indicative of cortical myoclonus in the reciprocally antagonist muscles. (C) Jerk-locked averaging analysis shows a positive-negative potential, recognizable over the left centroparietal electrodes, preceding myoclonus about 30 ms (right wrist extensor muscle; number of triggers = 100). Somatosensory evoked potential (SEP) and C-reflex following electric stimulation of the right median nerve at wrist showing large N20 component and the complex N20-P25 of the left centro-parietal region (upper trace) followed from C-reflex in right flexor radialis carpi muscle (lower trace). (D) 1H-MR spectroscopy using a PRESS sequence (TR 1500 ms, TE 144 ms) showing abnormal spectral peak areas at 3.22 ppm corresponding to choline (location of the 8 cm3 voxel: right cerebellar hemisphere). (Contributed by Dr. Pasquale Striano.)