Developmental Malformations
Prader-Willi syndrome
May. 10, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
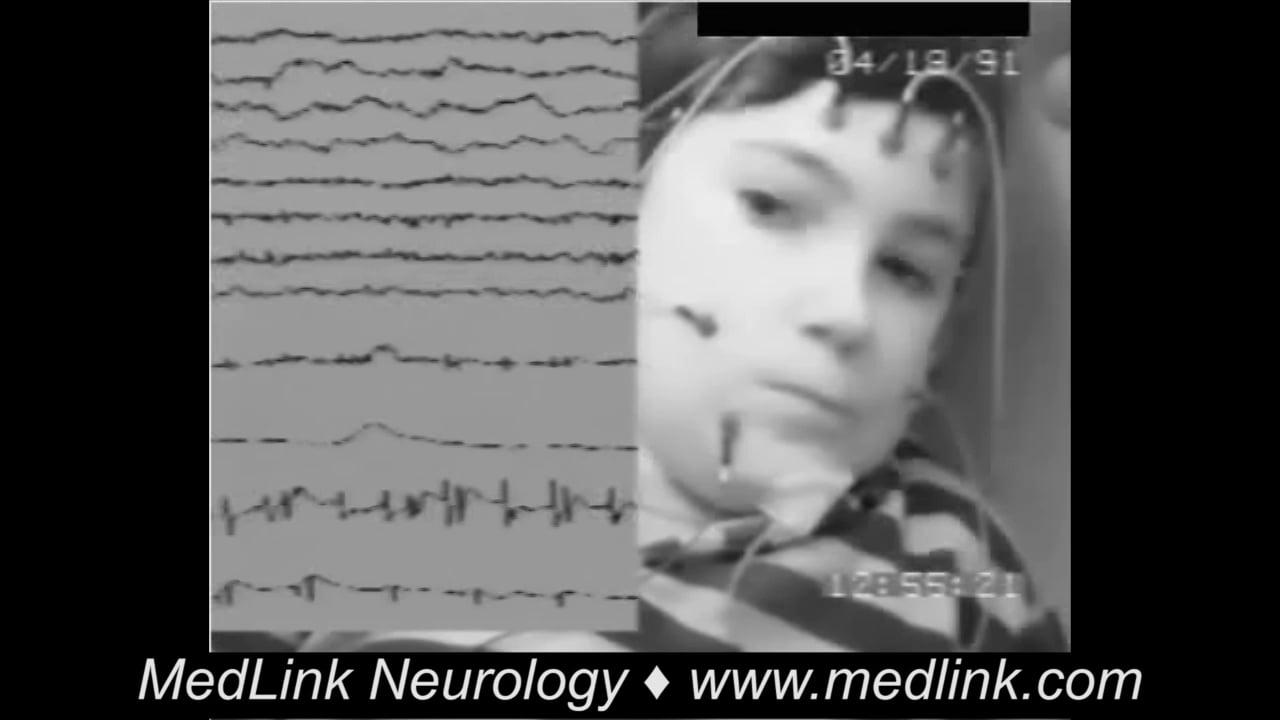
Interictal EEG (top) showing typical abandoned centrotemporal spikes. Ictal EEG started in the right central and midtemporal regions with 2- to 3-Hz slow waves and irregular, random, and monophasic medium-voltage spikes intermixed and superimposed on the slow waves (middle and bottom). This activity tended to spread, and the amplitude of the spikes rapidly increased before the first clinical manifestation, which occurred 30 seconds from the onset of the EEG ictal changes. The clonic phase was characterized by generalized polyspikes interrupted by slow waves at 5 to 7 Hz, which gradually slowed to 4 to 5 Hz, and finally to 1 to 2 Hz. The polyspike discharges were maximal posteriorly, with some right-sided emphasis. The electrical event of polyspikes and slow wave at 1 to 1.5 Hz continued for 60 seconds after the cessation of the clinical events. Used with permission: Panayiotopoulos CP. The Epilepsies: Seizures, Syndromes and Management. Oxford: Bladon Medical Publishing, 2005.