Epilepsy & Seizures
Febrile seizures
Jan. 23, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
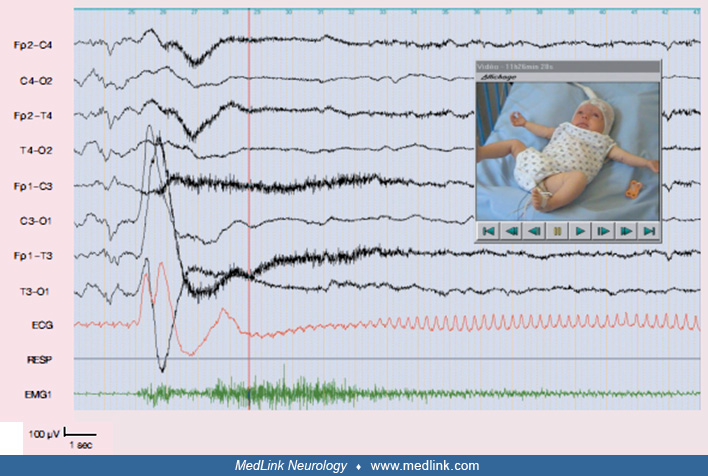
This 10-year-old girl with severe structural Lennox-Gastaut syndrome from age 6 months had a marked neuronal migration deficit in the right hemisphere, and her seizures were multiform and intractable to any medication. (A) A grossly abnormal interictal EEG with continuous, high-amplitude, sharp-slow-waves or spike-slow-waves. These were multifocal right or left, mainly frontal but also midline or posterior. (B) A tonic seizure started clinically with a scream (black arrow) and episodic nystagmus (red arrows show the eye movement artefacts of the nystagmus). The ictal EEG consisted of an abrupt onset of flattening, which lasted for 25 seconds, followed by high-amplitude, generalized, sharp and slow waves at approximately 1 Hz. The EEG returned to its preictal state after about 1 minute from the onset of the seizure. Despite unilateral structural abnormalities, the interictal, ictal, and postictal EEG abnormalities were not consistently lateralized. (Courtesy of C P Panayiotopoulos: Panayiotopoulos CP. A Clinical Guide to Epileptic Syndromes and Their Treatment. Revised 2nd ed. London: Springer, 2010.)