General Child Neurology
Extracerebral fluid collections in infants
Jan. 19, 2021
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
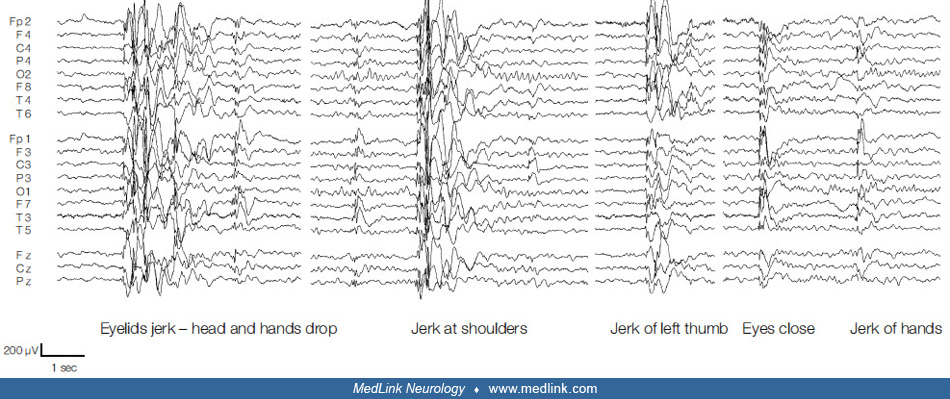
The background activity is normal, but there are frequent (at least every 10 seconds) 3 to 6 Hz generalized spike/polyspike-waves with anterior maximum; they are brief for 1 to 4 seconds. These are frequently associated with single jerks of mainly the shoulders but also, on other occasions, of the thumb or eyelids. The jerks occur simultaneously with the first or the second polyspike-wave complex of the discharges. Some jerks are followed by atonic attacks. The EEG also showed brief (shorter than 0.5 seconds) abortive 1.5 Hz generalized spike/polyspike-waves with anterior maximum and an alternating but not consistent side emphasis. There were no clinical manifestations. The paroxysmal discharges occurred with eyes opened and closed, spontaneously and during overbreathing. IPS did not evoke photoparoxysmal responses. (Courtesy of Dr. C P Panayiotopoulos 2010.)


