Epilepsy & Seizures
Focal seizures with experiential symptoms
Mar. 05, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
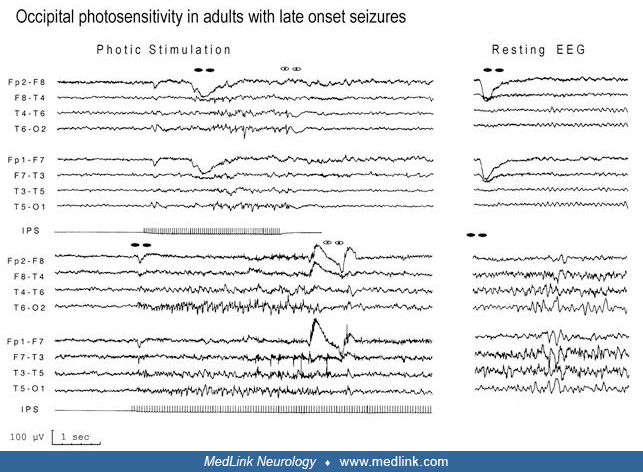
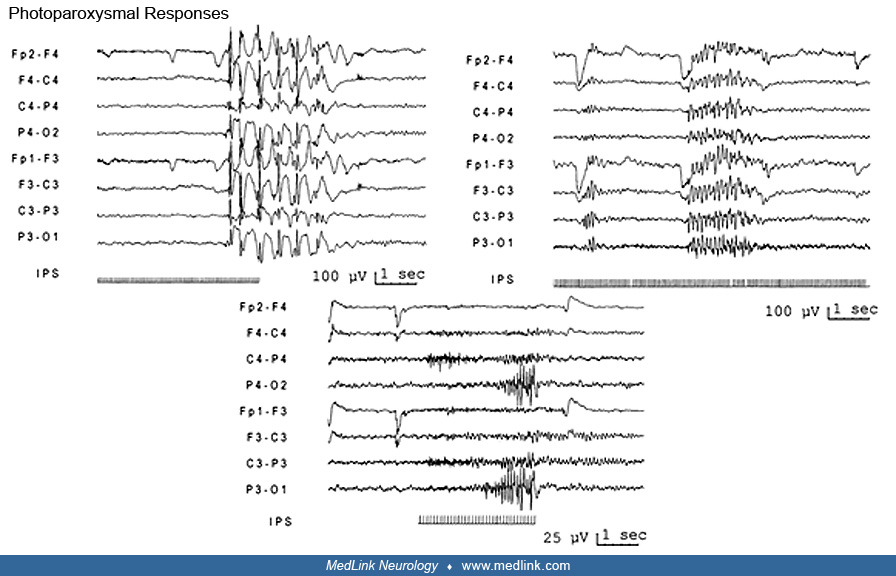
(Top) Generalized 3 to 4 Hz spike/polyspike-waves associated with an absence. The discharge outlasts the duration of the stimulus. (Middle) Generalized polyspike discharge in a patient with symptomatic spontaneous and photically induced mainly GTCS, which are resistant to appropriate antiepileptic medication. This type of discharge is usually associated with myoclonic jerks, which did not feature in this case. Note that the discharge occurs only after eye-blinks or eye-closure and does not outlast the stimulus train. (Bottom) Typical occipital spikes time-locked to each flash of intermittent photic stimulation. The patient is a woman with idiopathic occipital epilepsy (probably a variant of Gastaut-type childhood occipital epilepsy) who never had attacks precipitated by lights (Agathonikou et al 1997). (Used with permission from: Panayiotopoulos CP. Reflex seizures and related epileptic syndromes: a clinical guide to epileptic syndromes and their treatment. Revised 2nd ed. London: Springer, 2010:497-531.)