Movement Disorders
Akathisia
Jun. 19, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
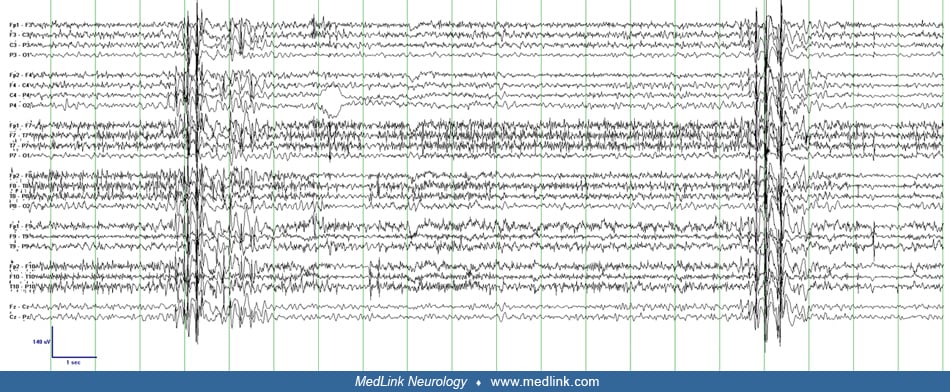
This 65-year-old woman had mild mental retardation and epilepsy with myoclonic-atonic seizures since childhood. Seizures had been infrequent for many years. In the setting of withdrawing levetiracetam, she developed frequent myoclonic jerks characterized by sudden flexion of her trunk and neck with abduction of her shoulders and arms. The patient was able to talk and interact with examiners between jerks. EEG background mild diffuse slowing with 10 Hz alpha rhythm and frequent 4 to 5 Hz bifrontally predominant polyspike-wave discharges corresponding to the myoclonus. Myoclonic jerks continued frequently (10 to 25 per hour) for 24 hours. This improved dramatically with reinstitution of levetiracetam. (Reproduced with kind permission of Springer Science+Business Media: Gerard E, Hirsch L. Generalised myoclonic status epilepticus. In: Panayiotopoulos CP, editor. The Atlas of Epilepsies. Springer, 2010.)