Sleep Disorders
Insufficient sleep syndrome
Jun. 14, 2024
MedLink®, LLC
3525 Del Mar Heights Rd, Ste 304
San Diego, CA 92130-2122
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Toll Free (U.S. + Canada): 800-452-2400
US Number: +1-619-640-4660
Support: service@medlink.com
Editor: editor@medlink.com
ISSN: 2831-9125
Nearly 3,000 illustrations, including video clips of neurologic disorders.
Every article is reviewed by our esteemed Editorial Board for accuracy and currency.
Full spectrum of neurology in 1,200 comprehensive articles.
Listen to MedLink on the go with Audio versions of each article.
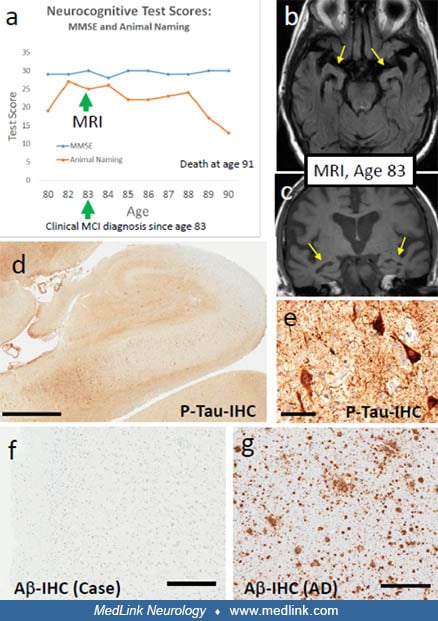
The subject was followed for 11 years from normal status until death at 91 years of age. Results of longitudinal neurocognitive tests are shown (a), including the Mini-Mental State Examination (MMSE) for global cognitive function and the Animal Naming Test (which is more sensitive for cognitive impairment). Note that the patient maintained high MMSE score, but there was evidence of progressive impairment according to the Animal Naming Test. At age 83 years, he was diagnosed with mild cognitive impairment, and MRI was obtained (b, c). These images showed evidence of brain atrophy, particularly in the medial temporal lobe and hippocampi (yellow arrows). The patient died from lung cancer at age 91 years. Autopsy results (d-f) showed neurofibrillary pathology in the hippocampus (d, e), but complete lack of brain Abeta amyloid (Abeta immunohistochemistry is shown from the middle temporal gyrus, representative of what was also observed in the frontal, parietal, and occipital neocortex as well as the hippocampus). For comparison, an Abeta immuno-stained Alzheimer disease brain is shown (g). Neuropathologic diagnosis was "PART, Definite." Scale bars = 2 mm (d), 50 microns (e), 200 microns (f, g). (Contributed by Dr. Peter Nelson.)